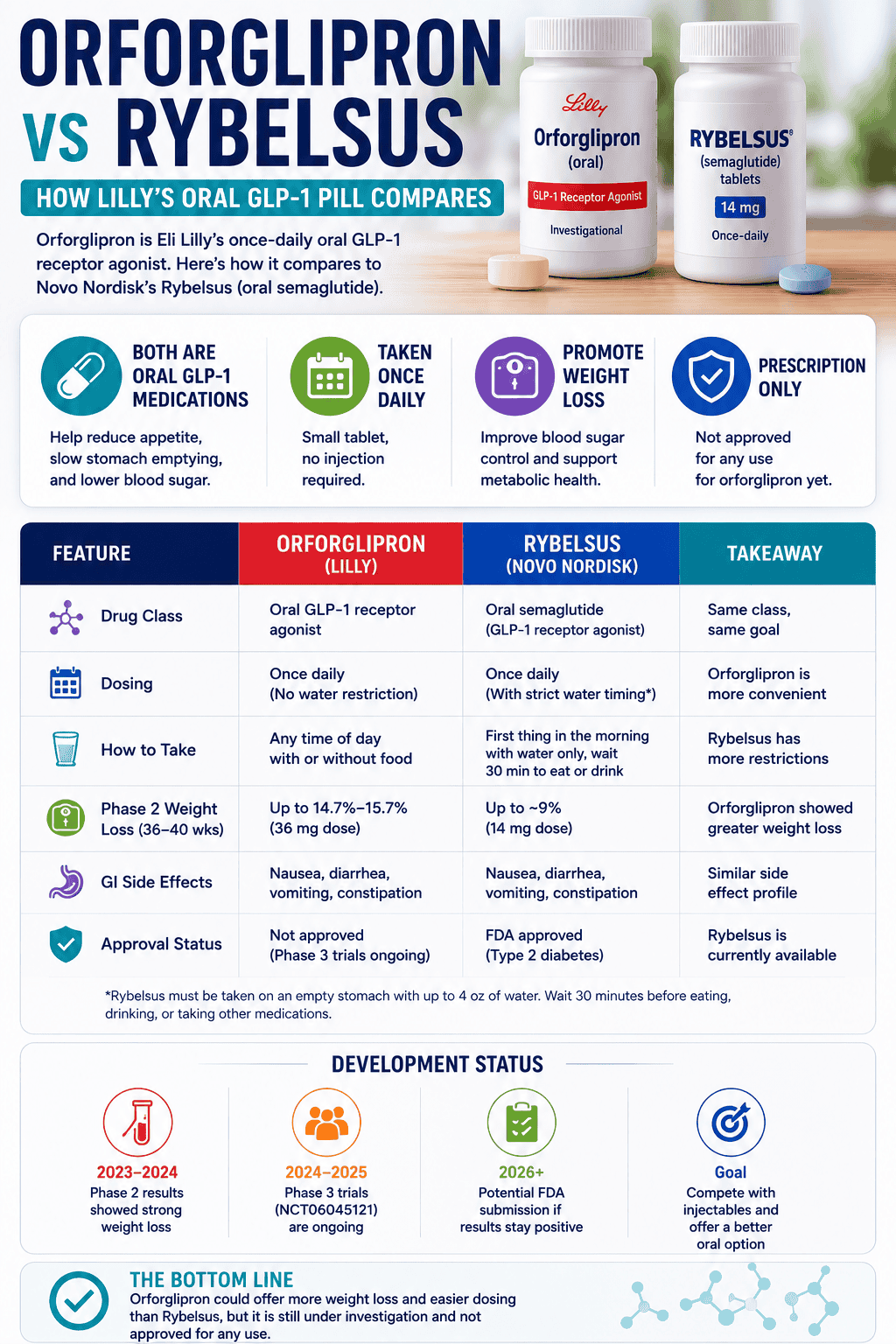
Electrolytes Explained: Sodium, Potassium, and Magnesium (When Each One Actually Matters)
Direct answer: electrolytes aren’t interchangeable. Sodium is mainly about fluid volume and pressure stability. Potassium is mainly about cellular electrical balance. Magnesium is mainly about nervous system and muscle downshifting. Most “electrolyte failures” happen when you treat them like one thing.
This page is the “what each one does” breakdown—so you can choose the right lever (and stop guessing with bundled mixes).
Which electrolyte do I need: sodium, potassium, or magnesium?
Start with your dominant signal. Electrolytes overlap in symptoms, but the “main story” is usually clear: sodium = volume stability, potassium = electrical stability, magnesium = downshift and relaxation. This page owns one intent: helping you choose the right lever based on the signal.
| Your intent | Most likely lever | Best first move | Common mistake |
|---|---|---|---|
| Dizziness on standing, low BP feelings, “dehydrated” despite drinking water | Sodium (volume) | Target sodium with fluids; test in a clean window | More water without sodium |
| Cramps, weakness, “heavy legs,” muscle instability | Potassium (electrical) | Increase dietary potassium; check meds first | Jumping to high-dose potassium supplements |
| Tension, twitching, poor sleep, can’t downshift | Magnesium (downshift) | Use a tolerable form; slow titration | Stopping early due to GI issues |
| Headaches after sweating, heat, or high water intake | Sodium (often) | Rebalance sodium + fluids; avoid dilution | Assuming it’s “low magnesium” by default |
- Kidney disease or reduced eGFR: potassium and magnesium supplementation require clinician oversight.
- Heart rhythm issues or concerning palpitations: don’t self-treat; electrolytes can be part of serious conditions.
- Diuretics, ACE inhibitors/ARBs, spironolactone: these can shift sodium/potassium balance significantly.
- Very high blood pressure or salt-sensitive hypertension: sodium strategy changes.
- Recent vomiting/diarrhea, heat illness, endurance events: losses can be large and fast—treat as higher stakes.
What do electrolytes actually do in the body?
Electrolytes help your body manage fluid distribution and electrical signaling. Sodium is the main regulator of extracellular fluid volume. Potassium is the major intracellular electrolyte that supports normal cell function and electrical gradients. Magnesium participates in many enzymatic processes and is commonly used for relaxation-focused goals.
How do I know if I need more sodium?
Sodium is the first lever when your symptoms look like volume instability: lightheadedness when standing, dehydration feelings despite water, headaches around sweating, or fatigue that improves when you hydrate correctly. The common trap is drinking lots of water without matching sodium.
- Dizziness or “gray-out” feeling when you stand up
- Headaches after sweating, heat, or high water intake
- Low blood pressure tendencies
- Symptoms improve when you add sodium with fluids (not just water)
How do I know if I need more potassium?
Potassium is a strong candidate when your symptoms feel like muscle and nerve electrical instability: cramps, weakness, flat output, or “heavy legs,” especially when diet is low in potassium-rich foods. Potassium deserves extra respect because supplementation can be risky in certain medical contexts.
- Cramps or muscle weakness (especially around activity or sweating)
- Constipation plus fatigue/weakness can occur in low potassium states
- Palpitations can happen for many reasons—treat as caution, not a DIY diagnosis
- If you take ACE inhibitors/ARBs or have kidney disease, do not supplement potassium without clinician guidance
How do I know if I need more magnesium?
Magnesium is the most common “downshift” lever: tension, twitching, poor sleep, and a nervous system that won’t settle. The confusion happens when magnesium is used to solve a sodium/potassium problem (or when the magnesium form causes GI issues and the test ends early).
Can drinking too much water mess up electrolytes?
It can. High water intake without adequate sodium can push you toward dilution—especially if you’re also sweating or eating a low-salt diet. That’s why some people feel worse when they “hydrate more” without changing electrolyte intake.
Electrolyte troubleshooting: how to tell it’s working
Electrolytes “work” when your target symptom improves predictably in the context that triggers it (heat, sweating, low-salt diet, heavy training). The biggest reason people stay confused is they change too many things at once.
- Using a “kitchen sink” electrolyte mix (you never learn which lever mattered)
- Adding potassium supplements without checking meds/health context
- Treating magnesium as the answer to volume instability (or vice versa)
- Judging results in one day without a repeatable trigger
- Pick one lever (sodium or magnesium first; potassium usually via diet first).
- Keep everything else stable for the week (caffeine, training spikes, sleep schedule).
- Test in the same context (same workout time, same heat exposure, same fluid intake pattern).
- Make one change after day 7 only if your metrics haven’t moved.
- Stop early if symptoms feel dangerous or worsen significantly.
- Sodium test: less dizziness on standing; fewer heat/sweat headaches; steadier energy in the trigger context.
- Potassium test (dietary): fewer cramps/weakness episodes over 1–2 weeks (assuming training is stable).
- Magnesium test: improved downshift (sleep latency/tension), fewer twitch/tension signals over 7–14 days.
- What not to expect: instant fixes if illness, anemia, sleep apnea, or medication effects are the main driver.
- Confusion, fainting/near-fainting, severe weakness, or chest pain
- Concerning palpitations, severe cramps with weakness, or symptoms that escalate fast
- Persistent vomiting/diarrhea or signs of dehydration that don’t improve
- Known kidney disease or heart disease without clinician guidance
Selected Professional References
- MedlinePlus Medical Encyclopedia: Low blood sodium (hyponatremia)
- NIH Office of Dietary Supplements: Potassium (Health Professional)
- MedlinePlus Medical Encyclopedia: Low blood potassium (hypokalemia)
- NIH Office of Dietary Supplements: Magnesium (Health Professional)
- Kardalas E et al. Hypokalemia: a clinical update (PMC)
Go Deeper (VerifiedSupps Guides)
Final Takeaway
Electrolytes aren’t one supplement category—they’re different levers. If you feel worse after “hydrating,” think sodium + fluids. If cramps and weakness dominate, think potassium (usually diet-first). If tension and poor sleep dominate, think magnesium. Pick one lever, run a clean 7–14 day test, and let the signal teach you.