By VerifiedSupps Editorial Team
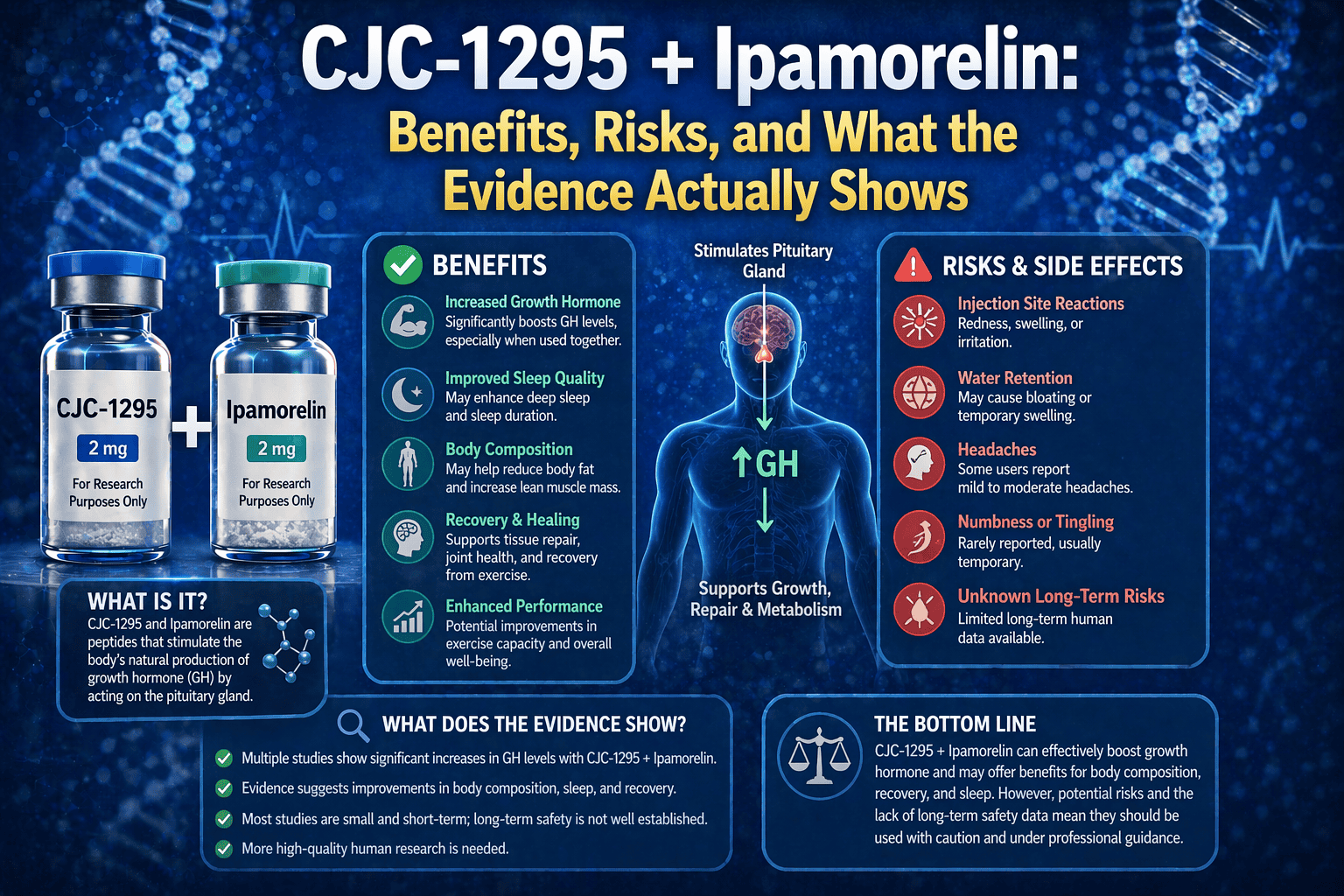
CJC-1295 + Ipamorelin: Benefits, Risks, and What the Evidence Actually Shows
CJC-1295 plus ipamorelin is one of the most common peptide stacks online for “growth hormone optimization.” It is usually pitched for better sleep, better recovery, more muscle, less fat, and anti-aging. The actual evidence is much narrower than that sales language makes it sound.
The strongest human evidence here is endocrine, not lifestyle-outcome based. CJC-1295 has human data showing sustained increases in growth hormone and IGF-1. Ipamorelin has older human pharmacology showing that it is a selective growth hormone secretagogue. What is still missing is a strong modern trial base proving that the combined stack reliably improves body composition, sleep, recovery, or aging outcomes in normal users.
This page is for the real question: how the stack is supposed to work, which claimed benefits are at least somewhat supported, what gets overextended, and why the safety and anti-doping picture still should make people slow down.
Key terms: CJC-1295, CJC-1295 DAC, ipamorelin, GHRH analogue, growth hormone secretagogue, ghrelin receptor, IGF-1, sleep, body composition, anti-doping
Quick Take
The best honest case for CJC-1295 plus ipamorelin is that it is a plausible GH-secretagogue stack, not a proven body-recomposition or anti-aging therapy. The strongest direct human signal is hormonal, not “more muscle, less fat, better sleep, better recovery” in a robust outcomes sense.
TL;DR decision
CJC-1295 plus ipamorelin may stimulate growth-hormone-related signaling, but the combined stack is marketed far beyond what strong human evidence really proves. The safest current read is “interesting endocrine stack with incomplete benefit and safety evidence,” not “proven physique, recovery, sleep, and longevity protocol.”
Evidence standard: human trials, dose ranges, guideline-level sources when available
Who this is for: people hearing about CJC-1295 and ipamorelin for sleep, fat loss, muscle gain, recovery, or anti-aging and wanting a cleaner evidence-based read
Who this is not for: anyone looking for gray-market sourcing, injection protocols, or reassurance that a non-approved peptide stack is already medically settled
Reviewed by: VerifiedSupps Editorial Team
Last reviewed: April 20, 2026
Parent Hub
VerifiedSupps Articles
Use the broader article hub if you want a calmer framework before assuming every hormone-related peptide stack is equally proven.
Quick decision table: what is actually supported?
This is the fastest way to separate hormonal plausibility from overstated lifestyle claims.
| If your real goal is… | Best current answer | Why | Best honest framing |
|---|---|---|---|
| Increasing GH and IGF-1 signaling | Plausible | CJC-1295 has human data showing prolonged GH and IGF-1 stimulation, and ipamorelin has human pharmacology showing selective GH secretagogue activity | The strongest evidence lane |
| Proven fat loss or muscle gain from the stack itself | Weak | The strongest human studies people cite are separate compound studies, not robust modern combo-outcome trials | Mostly extrapolated |
| Better sleep and recovery | Possible but not strongly proven | Direct human sleep and recovery evidence is not robust, and one older human study argued against a clear GHRP-axis role in slow-wave sleep regulation | Biologically plausible, not clearly proven |
| Safe, normal, medically settled use | No | FDA flags both compounds for compounding safety concerns, and both are prohibited in sport | Still an unsettled risk story |
Best next step (today): Ask whether the claim is about hormone signaling or about real-world outcomes. The evidence is much stronger for the first than the second.
Does CJC-1295 + ipamorelin actually work?
It likely works in the narrow sense of stimulating growth-hormone-related signaling. It is much less clearly proven in the broader sense people usually care about, like better body composition, better recovery, better sleep, or anti-aging outcomes from the stack itself.
The strongest direct human evidence here centers on CJC-1295. In healthy adults, subcutaneous CJC-1295 produced sustained, dose-dependent increases in GH and IGF-I, and mean IGF-I stayed elevated for 6 days or more after a single injection. Ipamorelin’s older human PK/PD work supports that it can trigger GH release, but that still is not the same thing as strong modern outcome data for the combination.
Mechanism
- CJC-1295 is a long-acting GHRH analogue intended to stimulate the pituitary through the GHRH pathway.
- Ipamorelin is a GH secretagogue acting through the ghrelin or GHS pathway and was developed as a relatively selective GH releaser.
- That is why people stack them: the idea is dual-pathway stimulation of endogenous GH release, not exogenous GH replacement.
What would change my recommendation: modern controlled human trials of the combination that actually measure body composition, sleep, recovery, and function instead of hormone changes alone.
Is all CJC-1295 the same, and what does ipamorelin add?
No. This is one of the most important details that gets flattened online. FDA’s 2024 compounding briefing says there are inconsistent naming conventions associated with CJC-1295-related bulk drug substances and notes that this can create a real safety risk because patients may be dosed with a different substance than intended.
The same FDA briefing distinguishes between two active moieties being evaluated: CJC-1295 and CJC-1295 DAC. It explains that CJC-1295 DAC includes a maleimidopropionamide-lysine unit at the C-terminus, while another form is synthesized without DAC. That matters because “CJC-1295” is often talked about online like a single clean product when it may not be.
Ipamorelin’s role in the stack is simpler: it is the ghrelin-pathway GH secretagogue layered on top of the GHRH-style stimulation from CJC-1295. So even the stack logic depends on knowing which CJC-1295 version is actually being discussed.
What benefits are most plausible with CJC-1295 + ipamorelin?
The most plausible benefits are the ones closest to the endocrine mechanism: higher GH-related signaling and higher IGF-1. The farther you move away from that core — especially into physique, anti-aging, and lifestyle claims — the weaker the human evidence gets.
Most plausible
Raising GH and IGF-1 signaling for a period of time. That is the clearest direct human signal in this whole stack discussion.
Moderately plausible
Supportive effects on body composition or recovery in some settings, but mostly by extrapolation from hormone biology rather than strong direct combo-trial proof.
Weakly proven
Reliable anti-aging, major muscle gain, major fat loss, or consistently better sleep from the stack itself.
That is the honest hierarchy: endocrine plausibility first, meaningful lifestyle-outcome proof second. And that second layer still is not very mature.
What do the human studies actually show about sleep, body composition, and recovery?
This is where the stack gets much shakier. The direct human evidence most often cited for CJC-1295 plus ipamorelin is mostly endocrine, not lifestyle-outcome based. Even the sleep story is less convincing than marketing usually suggests.
One older human study found evidence against a role of the GHRP axis in human slow-wave sleep regulation. That does not prove no one ever sleeps better while using a GH-secretagogue stack. But it does mean the simple “ipamorelin improves sleep because it’s a secretagogue” story is not strongly proven in humans.
The fairest interpretation is that sleep, recovery, and body-composition claims remain plausible extensions of GH-axis biology, not strong direct human outcomes already nailed down for this exact stack.
What are the biggest risks and side effects with CJC-1295 + ipamorelin?
The biggest risk is not just “unknown long-term safety” in the abstract. It is the combination of incomplete evidence, injectable-route risk, product-quality uncertainty, and a hormone axis that is not trivial to manipulate casually.
CJC-1295 risk signal
FDA says compounded CJC-1295 may pose immunogenicity risk for certain routes, may involve peptide-related impurities and characterization problems, and has identified serious adverse events including increased heart rate and systemic vasodilatory reaction. Available clinical data are limited.
Ipamorelin risk signal
FDA says compounded ipamorelin acetate may pose immunogenicity risk, is complicated by unnatural amino acids and peptide impurities, and notes published serious adverse events including death when ipamorelin was given intravenously for gastric motility.
That does not prove every use of these compounds will cause harm. But it does mean the current safety story is nowhere near relaxed enough to treat the stack like a routine wellness upgrade.
Is CJC-1295 + ipamorelin banned in sport or legally unsettled?
Yes on both counts in the way most people mean the question. Under the current anti-doping framework, CJC-1295 is prohibited as a growth hormone releasing factor and ipamorelin is prohibited as a growth hormone secretagogue or mimetic. That means the stack is banned at all times in sport.
USADA also states that CJC-1295 and ipamorelin are not approved for human clinical use and that their use poses significant health risks for athletes. FDA’s current compounding-risk materials reinforce that these are still substances with incomplete safety understanding rather than settled routine medicines.
So the cleanest answer is: not a normal approved medical stack, and definitely not sport-safe.
What should you do if you are thinking about CJC-1295 + ipamorelin?
The safest move is to stop treating “it boosts GH” as the end of the conversation. That is where the real-world evidence discussion should start, not stop.
Common mistakes
- Treating endocrine plausibility like proof of better sleep, body composition, recovery, and anti-aging.
- Ignoring that most human evidence centers on the individual compounds, not a strong controlled trial base for the combination itself.
- Treating a sports ban as proof that the benefits must already be dramatic.
- Treating gray-market injectable quality as a minor detail instead of a central safety issue.
Clean test protocol
| Inputs | A clear goal, a clear understanding of what is hormonal evidence versus actual outcome evidence, and a realistic appreciation that safety and source quality remain unresolved |
|---|---|
| Duration | Reassess when stronger controlled human studies of the combination actually exist. Until then, the most responsible posture is watchful skepticism. |
| 3 metrics | Whether the evidence is hormonal or functional, whether the stack itself was studied, and whether the source and route are medically legitimate |
| Stop conditions | Any gray-market sourcing, any blurred explanation of approval status, or any decision based mainly on marketing or forum confidence rather than controlled human outcomes |
How to tell it’s working
Right now, the better test is whether your framework got cleaner. A good evidence-based read should leave you less impressed by the phrase “GH secretagogue stack” and more focused on the difference between hormone changes and actual meaningful outcomes.
Red flags / seek care
Seek medical care for chest pain, fainting, severe swelling, trouble breathing, persistent vomiting, major injection-site reactions, or any severe reaction after using an unverified peptide product. Treat uncertain source quality itself as a safety problem, not a technicality.
Selected Professional References
These are the most useful sources for understanding what each compound actually does, what the direct human evidence supports, and why the current safety and anti-doping story still matter.
CJC-1295 in Healthy Adults
The key human paper showing prolonged GH and IGF-1 stimulation after CJC-1295 administration.
Used for: strongest direct hormonal evidence in the stack
Ipamorelin, the First Selective Growth Hormone Secretagogue
The best source for why ipamorelin is discussed as a relatively selective GH secretagogue rather than a generic peptide.
Used for: secretagogue identity and mechanism context
Pharmacokinetic-Pharmacodynamic Modeling of Ipamorelin
Useful for the healthy-volunteer GH-response context with ipamorelin.
Used for: direct human pharmacology support for ipamorelin
Evidence Against a Role for the GHRP Axis in Human Slow-Wave Sleep Regulation
A useful reality check against lazy “secretagogue = better sleep” assumptions.
Used for: direct sleep skepticism
FDA Risk Language for CJC-1295 and Ipamorelin
The most important official source for why the current safety story is not relaxed or routine.
Used for: immunogenicity, impurity concerns, and limited clinical data
FDA PCAC Evaluation of CJC-1295-Related Substances
Useful for the current FDA view on naming confusion, DAC vs non-DAC distinction, and characterization risk.
Used for: why not all CJC-1295 is the same
WADA-Aligned Prohibited List Guide
The clearest current source naming both CJC-1295 and ipamorelin inside the prohibited growth-hormone-releasing and secretagogue categories.
Used for: sports-ban status of both compounds
USADA Peptide Sanction Summary
Helpful because it clearly states that CJC-1295 and ipamorelin are not approved for human clinical use and carry health-risk concerns for athletes.
Used for: approval-status and risk context
Go Deeper (VerifiedSupps Guides)
These are the best next reads if you want the peptide-evidence cluster to make more sense after this stack breakdown.
Are Peptides Safe?
Best next read if your real question is whether the whole peptide category deserves more caution than the marketing suggests.
TB-500 for Recovery
Helpful if you want another example of how peptide-recovery claims can outrun direct human proof.
BPC-157: What Does It Do?
Useful if you want another peptide case where biology is louder than mature human outcomes.
MOTS-c Peptide
Helpful if you want another example of a peptide where mechanism is louder than human proof.
Final Takeaway
CJC-1295 plus ipamorelin is best understood as a plausible hormone-signaling stack, not a proven all-purpose physique, recovery, sleep, or anti-aging protocol. The strongest direct human evidence is about GH and IGF-1 biology, not the full lifestyle-outcome package usually promised. The safety and regulatory picture also is much less comfortable than the marketing suggests. The cleanest conclusion is “interesting endocrine stack, incomplete evidence, real reasons for caution.”
FAQ
Does CJC-1295 plus ipamorelin actually work?
It likely works in the narrow sense of stimulating GH-related signaling, but it is much less clearly proven in the broader sense of reliable body-composition, sleep, recovery, or anti-aging outcomes from the stack itself.
What is CJC-1295 supposed to do?
CJC-1295 is a long-acting GHRH analogue intended to increase endogenous growth hormone and IGF-1 signaling.
What is ipamorelin supposed to do?
Ipamorelin is a growth hormone secretagogue that acts through the ghrelin or GHS pathway and is generally described as a relatively selective GH releaser.
What are the most plausible benefits of the stack?
The most plausible benefits are the ones closest to the endocrine mechanism: higher GH-related signaling and higher IGF-1. Claims about dramatic body recomposition, major sleep improvement, recovery acceleration, or anti-aging are less strongly proven.
Is there strong human evidence for the combination itself?
Not in a strong modern outcomes-based way. The best human evidence is mostly about the individual compounds, especially CJC-1295’s effect on GH and IGF-1, not robust trials of the stack itself.
What are the biggest risks with CJC-1295 and ipamorelin?
The biggest risks include incomplete long-term safety evidence, injectable-route concerns, immunogenicity and impurity issues in compounded products, and uncertainty around product quality and real-world harm.
Is CJC-1295 plus ipamorelin safe for normal medical use?
No, not in the sense most people mean. These are not routine FDA-approved mainstream anti-aging, physique, or sleep medicines, and FDA has highlighted safety concerns for compounded versions.
Is CJC-1295 plus ipamorelin banned in sport?
Yes. Under the current anti-doping framework, CJC-1295 is prohibited as a growth hormone releasing factor and ipamorelin is prohibited as a growth hormone secretagogue or mimetic.
Why do people think the stack works better than the evidence shows?
Because hormone-pathway plausibility gets blended with lifestyle claims like better sleep, more muscle, less fat, and anti-aging, even when direct controlled human outcome evidence for the stack is still weak.
What is the safest way to think about this stack right now?
Treat it as a plausible GH-secretagogue stack with incomplete benefit and safety evidence, not as a settled or routine body-composition or anti-aging therapy.
VerifiedSupps Medical Disclaimer
This content is for educational purposes only and is not medical advice. CJC-1295 and ipamorelin are not routine FDA-approved anti-aging, physique, sleep, or recovery therapies, and current compounded-product safety concerns are real. Hormonal plausibility should not be confused with proven clinical benefit. Do not use unverified injectable peptide products as a substitute for evidence-based medical care. Seek urgent medical care for chest pain, fainting, severe swelling, trouble breathing, persistent vomiting, or major injection-site reactions after any peptide use.