By VerifiedSupps Editorial Team
TB-500 vs Thymosin Beta-4: What’s the Difference, What They’re Used For, and What the Evidence Actually Shows
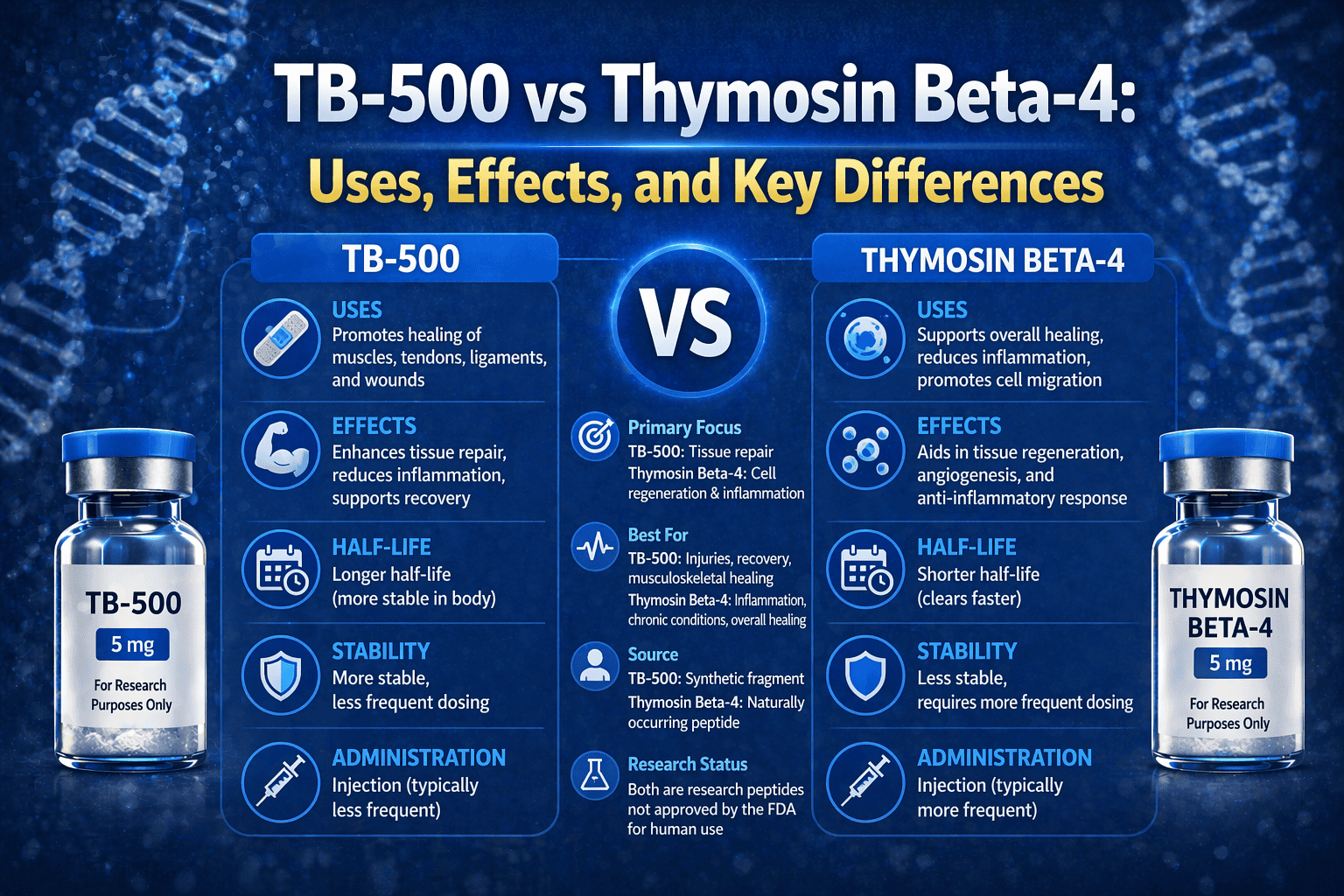
TB-500 and thymosin beta-4 are related, but they are not the same thing. Thymosin beta-4 is the full naturally occurring peptide or protein-sized peptide signal people usually mean when they talk about Tβ4 biology. TB-500 is generally described as a synthetic fragment derived from thymosin beta-4 biology, commonly linked to the short sequence LKKTETQ.
That difference matters because a lot of the more encouraging human clinical work in this broader area belongs to full-length thymosin beta-4 in topical eye or wound-healing settings, not to TB-500 as a musculoskeletal recovery injection. TB-500 keeps getting treated like it inherited all of thymosin beta-4’s evidence. It did not.
This page is for the real comparison: what TB-500 actually is, what thymosin beta-4 actually is, which one has real human data in which lane, and why those two things should not be casually blurred together.
Key terms: TB-500, thymosin beta-4, Tβ4, LKKTETQ, fragment peptide, wound healing, corneal healing, tendon recovery, sports ban, investigational peptide
Quick Take
Thymosin beta-4 is the broader, fuller biological story. TB-500 is the shorter synthetic fragment story. If you are talking about human evidence for eye healing, corneal repair, or some wound-healing applications, the stronger case belongs to full thymosin beta-4. If you are talking about the peptide most often marketed for tendon, muscle, or ligament recovery in gray-market circles, that is usually TB-500 — and the human proof there is much thinner.
TL;DR decision
TB-500 and thymosin beta-4 are connected, but they are not interchangeable. The most honest summary is: Tβ4 has the broader and somewhat more credible human clinical story, especially in topical healing contexts; TB-500 has the louder recovery hype but a weaker direct human evidence base.
Evidence standard: human trials, dose ranges, guideline-level sources when available
Who this is for: anyone trying to sort out whether TB-500 and thymosin beta-4 are the same thing, which one is actually used for what, and where the real evidence lives
Who this is not for: anyone looking for underground sourcing, injection protocols, or reassurance that a banned or unapproved peptide is “basically proven”
Reviewed by: VerifiedSupps Editorial Team
Last reviewed: April 17, 2026
Parent Hub
VerifiedSupps Articles
Browse the broader article hub if you want a calmer framework before assuming every peptide with a repair story is equally proven.
Quick decoder: TB-500 vs thymosin beta-4
This is the fastest way to understand what belongs to the full peptide story and what belongs to the fragment story.
| If you mean… | Best fit | Why | Best honest framing |
|---|---|---|---|
| The naturally occurring peptide tied to tissue repair biology | Thymosin beta-4 | It is the full endogenous peptide or protein-sized peptide signal used in most of the older biology and human topical-healing literature | Broader and more clinically grounded |
| The short synthetic fragment often marketed for recovery injections | TB-500 | It is generally described as a synthetic fragment derived from Tβ4, commonly associated with the acetylated 17–23 fragment LKKTETQ | Louder hype, weaker direct human proof |
| The stronger human eye-healing and wound-healing story | Thymosin beta-4 | Human trials and case-series data exist in dry eye, corneal healing, and wound-healing settings | More human signal, still not universal proof |
| The peptide usually discussed in sports bans and gray-market musculoskeletal recovery | TB-500 | TB-500 is the derivative most often named in WADA materials and most often sold into recovery culture | High visibility, lower certainty |
Best next step (today): If you are reading a benefit claim, ask whether the evidence came from full thymosin beta-4 or from TB-500 itself. That one question clears up most of the confusion.
What is the actual difference between TB-500 and thymosin beta-4?
The real difference is simple: thymosin beta-4 is the full endogenous peptide, while TB-500 is generally described as a synthetic fragment derived from thymosin beta-4 biology. They are connected, but they are not interchangeable.
That distinction matters because the full peptide and the fragment do not bring the same evidence package with them. A lot of the better-known human clinical work — especially in eye-surface disease and wound healing — belongs to full thymosin beta-4. By contrast, TB-500’s mainstream reputation comes more from sports, underground recovery use, and preclinical or theory-driven musculoskeletal narratives.
Mechanism
- Thymosin beta-4 is an endogenous peptide involved in cell migration, actin dynamics, wound healing, and repair-related biology.
- TB-500 is associated with the shorter acetylated fragment Ac-LKKTETQ, detected analytically as a thymosin beta-4 fragment.
- Borrowing the biology of the parent peptide does not automatically prove identical real-world effects for the fragment.
What would change my recommendation: cleaner human trials using TB-500 itself in well-defined musculoskeletal settings, rather than continued borrowing from thymosin beta-4 biology and topical clinical data.
What is thymosin beta-4 actually used for?
The best-supported human uses for thymosin beta-4 are in topical healing-related contexts, especially the eye and wound-healing lanes. That is the part of the story most people miss when they only know the peptide world through sports-recovery talk.
Dry eye and corneal healing
Phase 2 human work with topical thymosin beta-4 ophthalmic solution showed significant improvement in severe dry-eye signs and symptoms, and related literature supports a corneal-healing role.
Wound healing
Review-level sources summarize phase 2 work in pressure ulcers and stasis ulcers, with faster healing in patients who did heal, plus broader dermal-healing potential.
This is the cleaner medical lane for full thymosin beta-4: topical or wound-healing-oriented human use, not mostly the gym-recovery mythology that tends to dominate social media.
What is TB-500 actually used for?
In the real world, TB-500 is mostly used in recovery culture for tendon, ligament, muscle, joint, and “healing” goals. In the evidence world, though, that use case is much less settled than the marketing implies.
A recent orthopaedic review describes TB-500 as a synthetic fragment derived from thymosin beta-4 and notes repair-related preclinical signals, but also says human orthopaedic data are lacking. That is the main reality check. TB-500 is widely talked about for musculoskeletal recovery, but direct human proof in that lane still is not strong.
So the honest summary is this: TB-500 is used for recovery goals in practice, but those practical uses rest much more on theory, animal work, and peptide-culture confidence than on mature human musculoskeletal trial evidence.
Which one has stronger human evidence?
Thymosin beta-4, clearly. It is not because full Tβ4 is “fully proven” in every healing application. It is because the human evidence that does exist is much more concrete and clinically recognizable.
Thymosin beta-4
Human data exist in dry-eye disease, corneal healing, and wound-healing contexts. The evidence is still niche, but it is real and clinical.
TB-500
The fragment’s mainstream recovery reputation is much louder than its direct human musculoskeletal evidence. That is the key difference.
This is why people get misled. They hear that “thymosin beta-4 helps healing,” then assume TB-500 injections must therefore be strongly validated for tendons and muscles. That leap is exactly where the evidence gets overstated.
Are TB-500 and thymosin beta-4 safe?
Topical full thymosin beta-4 and compounded injectable TB-500 do not sit in the same safety category. That is probably the most important safety sentence in the whole article.
The full thymosin beta-4 clinical work in eye and wound-healing settings is still investigational, but it at least has recognizable human exposure. TB-500 is different. FDA’s current safety-risk page for “Thymosin Beta-4, Fragment (LKKTETQ)” says compounded drugs containing the fragment may pose immunogenicity risk for certain routes of administration due to aggregation and peptide-related impurities, and FDA says it has not identified any human exposure data for drug products containing the fragment.
That does not prove TB-500 is automatically dangerous in every context. But it does mean the confidence level should be much lower than many users assume, especially for gray-market injected products.
Why are both TB-500 and thymosin beta-4 banned in sport?
Because WADA’s 2026 prohibited list includes thymosin-β4 and its derivatives, with TB-500 named as an example. That means the regulatory sports view is already broader than “just the short fragment.”
This matters because some athletes or biohackers treat a ban as proof that a substance must work extremely well. That is not a sound conclusion. The sports-ban point tells you the category is restricted. It does not solve the human efficacy question in the exact use case you care about.
The best read is that sports regulators view the Tβ4 family and its derivatives as relevant enough to prohibit, but that still is not the same thing as saying TB-500 has a clean, mature clinical evidence base for recovery.
What should you do if you are comparing TB-500 and Tβ4?
The smartest move is to decide which lane you actually care about. If you care about the most credible human healing data, the better conversation is full thymosin beta-4 in topical eye or wound-healing settings. If you care about the peptide most often sold for tendon or muscle recovery, you are really talking about TB-500 — and you should be much more cautious with the confidence level.
Common mistakes
- Using thymosin beta-4 human data to prove TB-500 injection claims.
- Treating the fragment and the parent peptide like they are interchangeable molecules.
- Using the sports ban as if it were clinical efficacy proof.
- Ignoring FDA’s current concern about fragment-specific immunogenicity and lack of human exposure data for compounded TB-500 products.
Clean test protocol
| Inputs | A clear definition of the goal, a clear distinction between full Tβ4 and TB-500, and a willingness to rank human clinical data above peptide-culture certainty |
|---|---|
| Duration | Reassess when cleaner human TB-500 musculoskeletal studies actually exist. Right now the comparison is still asymmetrical. |
| 3 metrics | Whether the evidence is human or preclinical, whether it belongs to TB-500 or Tβ4, and whether the route of use matches the evidence source |
| Stop conditions | Any gray-market seller, any claim that the fragment is “the same thing” as the parent peptide, or any decision based mostly on anecdote and sports gossip rather than actual human data |
How to tell it’s working
Right now, the better test is whether your framework got cleaner. A good comparison should leave you less impressed by vague “healing peptide” language and more able to ask: which molecule, which route, which evidence base?
Red flags / seek care
Seek medical care for severe swelling, rash, trouble breathing, chest pain, fainting, or strong injection-site reactions after any unverified peptide product. And treat uncertain source quality as its own safety problem, not a minor detail.
Selected Professional References
These are the key sources behind the fragment-vs-parent distinction, the human healing data for full Tβ4, the limited evidence for TB-500, and the current safety and sports-ban context.
Therapeutic Peptides in Orthopaedics
One of the clearest current summaries that TB-500 is treated as a synthetic fragment derived from Tβ4 and that human orthopaedic data are still lacking.
Used for: TB-500 identity and limits of musculoskeletal human data
Identification of the N-Terminal 17–23 Thymosin Beta-4 Fragment in TB-500
The most useful source for why TB-500 should not be casually treated as the same thing as full thymosin beta-4.
Used for: fragment identity and LKKTETQ context
Thymosin β4 Ophthalmic Solution for Dry Eye
A key human source showing where the fuller Tβ4 clinical story is actually strongest.
Used for: phase 2 dry-eye efficacy and human exposure context
Thymosin β4 Significantly Improves Severe Dry Eye
Another strong human Tβ4 reference that lives in the topical eye-healing lane, not the gray-market recovery lane.
Used for: confirming the fuller Tβ4 eye-healing story
The Regenerative Peptide Thymosin β4 Accelerates Wound Healing
Helpful because it ties together the fuller Tβ4 wound-healing clinical story and why it gets more medical respect than TB-500 does.
Used for: wound-healing clinical context
FDA Risk Language for Thymosin Beta-4 Fragment (LKKTETQ)
The most important official source for why fragment-based TB-500 should not be treated like a comfortable safety story.
Used for: immunogenicity, impurities, and lack of human exposure data
WADA Prohibited List
The key current source for why both thymosin-β4 and its derivative TB-500 matter in the anti-doping context.
Used for: current sports prohibition language
Go Deeper (VerifiedSupps Guides)
These are the best next reads if you want the peptide-recovery cluster to make more sense after the TB-500 vs Tβ4 distinction is clear.
Are Peptides Safe?
Best next read if your real question is whether the whole peptide category deserves more caution than the marketing suggests.
TB-500 for Recovery
Helpful if you want the direct TB-500 recovery claim broken down on its own after this comparison.
BPC-157: What Does It Do?
Useful if you want another example of how peptide-recovery hype often outruns human evidence.
MOTS-c Peptide
Helpful if you want a second example of a peptide where mechanism is louder than human proof.
Final Takeaway
TB-500 and thymosin beta-4 belong in the same family story, but not in the same evidence bucket. Thymosin beta-4 has the broader and more clinically recognizable healing record, especially in topical eye and wound settings. TB-500 is the louder recovery fragment in gym and peptide circles, but its direct human musculoskeletal proof is much weaker. The cleanest answer is not “one is good and one is fake.” It is “know which molecule you are talking about, know which route the evidence belongs to, and do not let the parent peptide’s credibility automatically upgrade the fragment.”
FAQ
Is TB-500 the same as thymosin beta-4?
No. Thymosin beta-4 is the full endogenous peptide, while TB-500 is generally described as a synthetic fragment derived from thymosin beta-4 biology and commonly associated with the short sequence LKKTETQ.
Which one has stronger human evidence?
Thymosin beta-4 does, especially in topical eye-healing and wound-healing settings. TB-500’s direct human musculoskeletal evidence is much thinner.
What is thymosin beta-4 mainly used for?
The strongest human clinical uses are in topical healing-related settings such as dry eye, corneal healing, and wound-healing contexts.
What is TB-500 mainly used for?
In practice, TB-500 is mostly used in recovery culture for tendon, ligament, muscle, and joint-healing goals, but the direct human proof in that lane is limited.
Why do people confuse TB-500 and Tβ4?
Because TB-500 is often marketed using the biology and reputation of full thymosin beta-4, which makes the two sound more interchangeable than they really are.
Is TB-500 safe?
The safety picture is not comfortable. FDA’s current risk language for the thymosin beta-4 fragment cites immunogenicity concerns, peptide-related impurities, and a lack of human exposure data for drug products containing the fragment.
Is thymosin beta-4 safer than TB-500?
Topical full thymosin beta-4 at least has more recognizable human clinical exposure than TB-500, but that does not make all Tβ4 uses broadly proven or risk-free. The key point is that topical full Tβ4 and injected TB-500 should not be treated like the same safety category.
Are TB-500 and thymosin beta-4 banned in sport?
Yes. WADA’s 2026 prohibited list includes thymosin-β4 and its derivatives, with TB-500 named as an example.
Does TB-500 have proven human tendon or muscle-healing data?
Not in a strong mature way. Current review-level sources say human orthopaedic data are lacking.
What is the safest way to think about the comparison?
Treat full thymosin beta-4 as the broader and somewhat more clinically grounded healing story, and treat TB-500 as the louder recovery fragment story with weaker direct human proof.
VerifiedSupps Medical Disclaimer
This content is for educational purposes only and is not medical advice. TB-500 and thymosin beta-4 are investigational peptide concepts, not normal retail supplements, and they should not be treated as equally proven or equally safe across routes of use. Topical full thymosin beta-4 clinical exposure is not the same thing as gray-market injected TB-500 use. Do not use unverified peptide products as a substitute for evidence-based diagnosis, rehab, or medical treatment. Seek urgent medical care for severe swelling, trouble breathing, chest pain, fainting, strong allergic-type reactions, or serious injection-site problems after any peptide use.